

Introduction: ARU-1801 is a gene therapy consisting of autologous CD34+ hematopoietic stem cells and progenitors (HSCPs) transduced with a lentiviral vector (LV) encoding a modified γ-globinG16D gene. Preclinical studies in SCD mice have shown that g-globinG16D binds α-globin with higher affinity; hence, the g-globinG16D LV produces 1.5-2x more HbF/vector copy number (VCN) than a g-globin LV. Preliminary studies also show greater reduction in reticulocytes in SCD mice expressing HbFG16D compared to those expressing the same level of HbF, suggesting that HbFG16D may have a more potent anti-sickling effect than HbF. We hypothesized a high potency anti-sickling globin would allow ARU-1801 to be effective with reduced intensity conditioning (RIC). RIC would result in lower toxicities and resource utilization compared to myeloablative approaches, allowing access of gene therapy to a broader group of SCD patients.
We previously reported early data from patient 1 (P1) and 2 (P2) in the ongoing Phase 1/2 study (NCT02186418), who were treated with drug product (DP) from the initial ARU-1801 manufacturing process (Process I). We now present the long-term data on these patients and early data from P3, the first patient treated with our new manufacturing process (Process II).
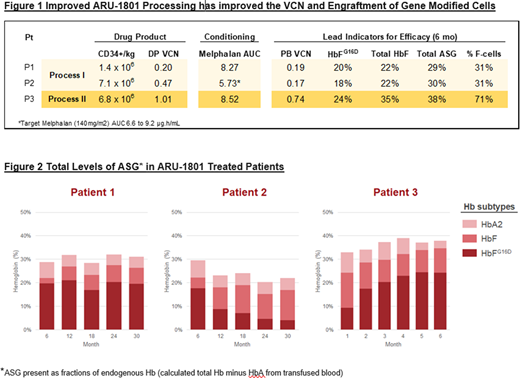
Methods: Adults with severe SCD, as defined by recurrent vaso-occlusive events (VOE) and acute chest syndrome deemed eligible were enrolled. Manufacturing process improvements in Process II included optimized timing of HSCP collection after plerixafor mobilization, LV production and improved HSCP transduction. Prior to DP infusion, all patients received a single dose of IV melphalan (140 mg/m2 BSA) and were weaned off transfusions 3-6 months after DP infusion. Patients were monitored for safety, engraftment, VCN, anti-sickling Hb (ASG) expression, and hematological and clinical manifestations of SCD. Levels of ASG (including HbFG16D) are presented as fractions of endogenous Hb.
Results: As of 28 July 2020, data from 3 patients treated with ARU-1801 are available. P1 (34yr old) has HbSβ0- and P2 (24yr old) has HbSβ+ thalassemia (2-3% HbA). Both have 30 months (mo) post-transplant (PT) follow up. P3 (19yr old) has HbSS genotype with 6 mo PT follow up. ARU-1801 demonstrated a favorable safety profile with no treatment-related adverse events to date. Time to neutrophil engraftment (ANC ≥500) was 9, 7, and 7 days PT, and time to platelet recovery (Plt >50,000) was 12, 7, and 6 days PT, in P1, P2, and P3, respectively. Figure 1 shows HSPC dose, conditioning exposure and gene transfer; Figure 2 shows ASG over time. Using Process I, P1 has shown stable expression of 20% HbFG16D, 31% ASG and 31%à64% F-cells over 2.5 years, despite a low DP VCN of 0.2 and low HSPC dose of 1.4 x106 cell/kg. P2 received a higher cell dose of 7.1 x106 cell/kg with a DP VCN of 0.47 but had below target melphalan exposure, likely due to rapid clearance from hyperfiltration (GFR= 200 mL/min/1.73m2). Despite lower engraftment and HbFG16D level, P2 maintains stable total ASG of 22% at 30 mo due to a compensatory increase in HbF. Using Process II, P3 received DP of 6.8 x106 cells/kg with a VCN of 1.0, and demonstrated an engrafted VCN of 0.74, 71% F-cells and 91% F-reticulocytes at 6 mo. As P3 is being weaned off transfusions, HbFG16D is progressively rising, showing the selective advantage to HbFG16D-containing RBCs. P1 and P2 have maintained improvements in VOEs, no VOE in P3 so far (data will be presented).
Conclusion: We show that engraftment of ARU-1801 and amelioration of disease is possible with RIC using IV melphalan, with persistent stable ASG expression and meaningful improvement in VOEs in P1 and P2. P1 shows stable HbFG16D and high ASG despite low, albeit stable VCN. P2 had lower HSCP engraftment, which we hypothesize was due to below target melphalan exposure. Nevertheless, significant clinical benefit was observed in P2 due to stable ASG of 22% at mo 30. It is likely that the presence of this amount of HbFG16D has provided enough ASG to prevent sickling/ineffective erythropoiesis, resulting in the preferential survival of HbF+HbFG16D-expressing RBC. Process II DP in P3 resulted in 2-4X higher engraftment of transduced HSCPs at 6 mo. Additional process enhancements are under development for future treated patients. ARU-1801, administered with RIC, holds significant promise for achieving durable responses with a favorable safety profile in patients with severe SCD.
Asnani:Aruvant Sciences: Research Funding; Avicanna Ltd.: Research Funding. Lutzko:Aruvant Sciences: Patents & Royalties: pre-clinical vector development. Lo:Aruvant Sciences: Current Employment. Little:Aruvant Sciences: Current Employment. McIntosh:Aruvant: Current Employment, Current equity holder in private company. Malik:Aruvant Sciences, Forma Therapeutics, Inc.: Consultancy; Aruvant Sciences, CSL Behring: Patents & Royalties.
Plerixafor - stem cell mobiliziation Melphalan - chemotherapy conditioning pre autologous transplant with ARU-1801

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal